Photo by Anna Shvets from Pexels
On Tuesday, August 11, just as Florida was setting a new daily record for deaths from Covid-19, Billy Woods, sheriff of Marion County in north central Florida, banned all of his employees, with a few exceptions, from wearing masks.
“This is no longer a debate,” he told his staff, explaining how he had considered his ruling carefully: “The fact is, [for] the amount of professionals that give the reason why we should, I can find the exact same amount of professionals that say why we shouldn’t.”
A large majority of health experts in fact think that wearing masks saves lives; but Wood is not alone in his willingness to sidestep expert opinion.
Across the country, adding insult to injury to an already underfunded and delegitimized federal Centers for Disease Control and Prevention (CDC), elected officials have stalled (and sometimes thwarted) efforts to develop COVID-19 testing capacity; they have foregone the necessary resources to develop a comprehensive national contact tracing program; and some have even discredited scientific claims about the scale of the pandemic and the kind of public health response that is necessary.
The graph below shows the tragic results. After flattening for a time, America’s death rate from the coronavirus has once again risen:
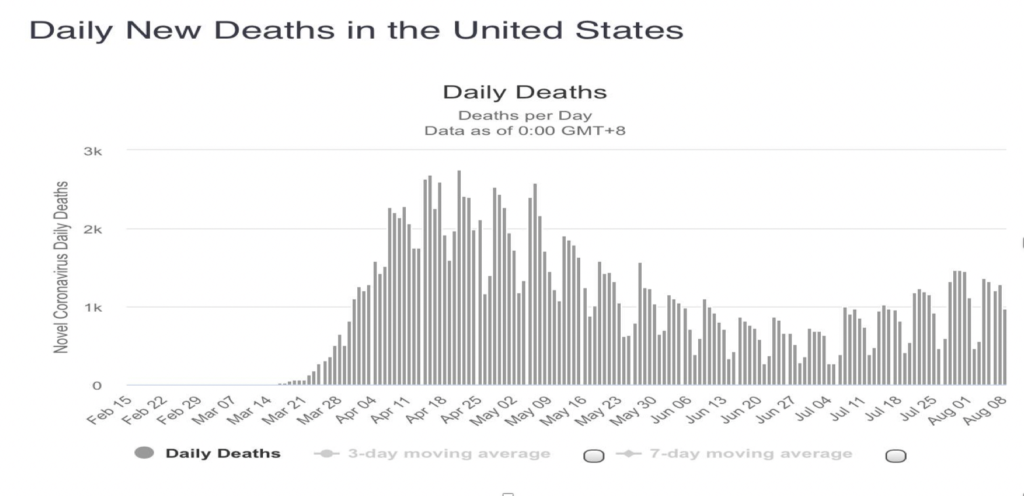
But why? Why has a country with rich resources and public health expertise failed to contain COVID-19?
An important part of the answer lies in our inability to learn from other countries’ experiences.
The nationalist exceptionalism promoted by “America First” is only the surface of the problem. We failed to see early enough that the source of our susceptibility to the virus was Europe – which was why the first “hotspot” was in New York City – and then we turned down other countries’ offers to collaborate. It was only in August that the President’s coordinator for the pandemic, Dr. Deborah Birx, admitted that we ought to have studied the measures taken by the Italian government in flattening the curve by a total lockdown.
A deeper, independent reason for our failure is the institutional fragmentation of the American public health system. As political scientists Scott Greer and Phillip Singer have pointed out in their analyses of prior public health emergencies, “few other countries have quite so many independent governments.” In the United States, competency over public health is spread across (and within) a dizzying array of local governments, counties, states, territories, and federal agencies. Competency, moreover, does not guarantee a clear demarcation of responsibility. Several levels of government can intervene legally in public health management, creating the potential for mixed messages, and conflicting orders from the sheriffs and other officials of different counties.
Acknowledging the challenges, some state governments have tried to cooperate, as a new ten-state testing strategy led by Maryland’s Republican governor, Larry Hogan, shows. But not always.
Grave intergovernmental disputes have also erupted, such as the legal battle over Covid policy between Georgia Governor Brian Kemp and Atlanta Mayor Keisha Lance Bottoms.
Worse still, when state governments choose not to exercise their authority over public health matters, affected Americans are left in a dangerous no-man’s-land. Legal scholars Jessica Bulman-Pozen and Heather Gerken refer to these pitfalls as the products of “uncooperative” federalism.
Why have other industrial nations been more effective in responding to the pandemic?
Common to their success has been the “Test, Trace, Treat” triumvirate of pandemic management. Almost invariably, an independent and centralized public health authority has been behind its implementation. Like central banks, these authorities are composed of specialists whose expertise in an area of public welfare exceeds that of most elected officials. These experts have intervened in public policy in cases where excessive political interference would be detrimental.
Consider the centralized health system in France.
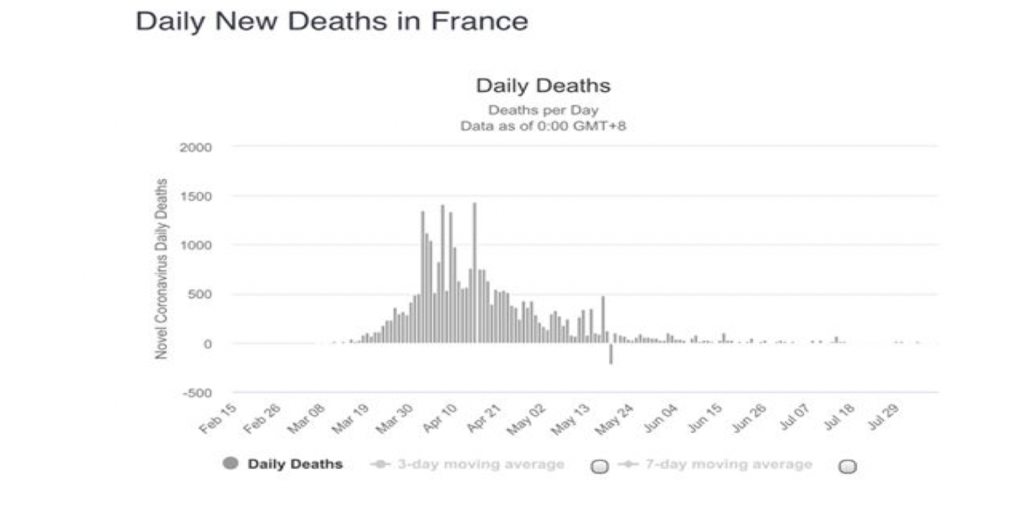
Like the US, France too had testing and treatment problems early on. But President Emmanuel Macron, unlike President Trump, has played an influential role in directing and controlling the coronavirus crisis through France’s centralized health authority. After completing a first round of lockdown, in July the French authorities followed scientific counsel and imposed a mandatory mask mandate for enclosed places to head off a “second spike” in cases. As a result, the country’s current trends in morbidity and mortality are largely positive, as the following graph reveals:
The current pandemic has exposed the staggering costs of American politicians’ undue influence over policies to combat the pandemic. Such influence was visible in the interactions between President Trump and CDC director Robert Redfield at the daily press briefings last spring. Rather than using the briefings as a forum in which to put forward a uniform message based on scientific advice, the President preferred to use them to deliver a political sales pitch. When the briefings failed to improve his standing in the polls and instead popularized infectious disease chief Anthony Fauci, Trump abruptly cancelled them and criticized Fauci, only to bring the briefings back as a campaign tool as the November election loomed.
But a decentralized public health system needn’t necessarily entail failure in facing a pandemic.
Consider Italy, whose regional governments stand in contrast to France’s centralized political system – but whose Prime Minister commands far more popular support than either the French or the American President.
In the early stages of Italy’s crisis, when there was no experience to guide them, Italy’s 20 regional health authorities panicked, filling their hospitals with victims with light symptoms, thus leaving less space for those who were badly stricken. As Walter Ricciardi, Scientific Director of the National Observatory in Health in the Italian Regions, has underlined, “the experience of the pandemic has shown that the decentralization of public health, beyond risking the equality of the citizens with respect to public health, was incapable of facing an emergency situation.”
Still, as the gravity of the situation and the inadequacy of Italy’s regional health systems were revealed, the Prime Minister declared a national state of emergency, and the National System for Civil Protection was tasked with taking over from the regional health structures. From that time on, all of Italy’s decisions relating to the pandemic — what to close, which activities to stop and for how long, what to open and in what order – have been made at the national level.
As is now well-known, Italians were totally locked-down for several months. All residents were required to have a certificate to travel between regions, cities, and even neighborhoods. All residents could be fined if they were found to be disobeying the rules. And in contrast to the United States, masks are compulsory in enclosed areas throughout Italy, and individuals who ignore the law face a 1,000 Euro fine.
Prime Minister Conte’s strategic emphasis on national solidarity boosted morale as well as his own popularity. As Jason Horowitz pointed out in the New York Times on August 1st, “European states that once looked smugly at Italy are facing new flare-ups….And Italy? Its hospitals are basically empty of Covid-19 patients.”
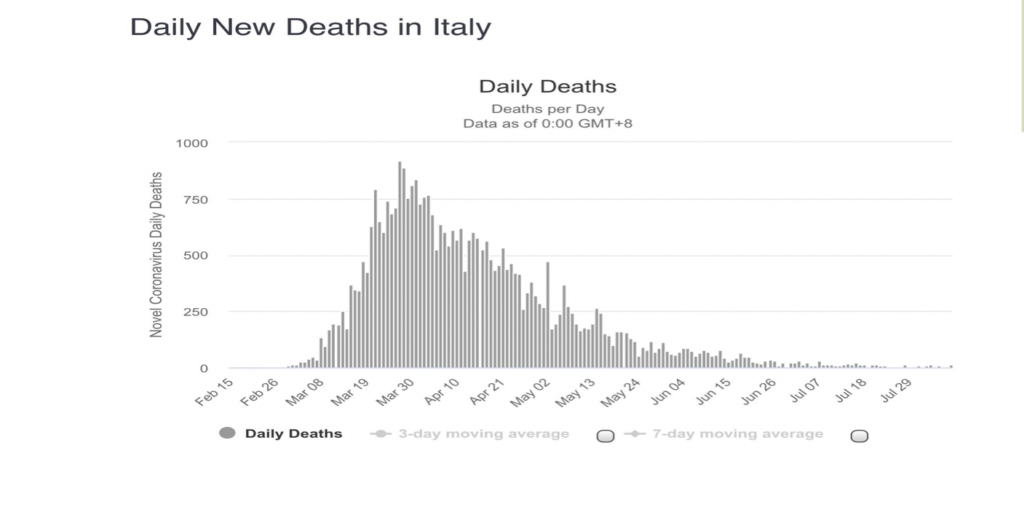
Italy is a good contrast to the United States because it started out so badly, but has had more success than many of its neighbors in combatting the virus. The decentralized and famously inefficient Italian regional institutions did not prevent the federal government from responding effectively.
As the following graph shows, these policies have lowered the death rate in Italy to close to zero.
In the US, in contrast with Italy, the abdication of national leadership has exacerbated the lack of coordination inevitable in a decentralized federal system. In its place appears what Jessica Bulman-Pozen has called “partisan federalism,” as different states followed contradictory policies, depending on which party controlled the state government. Just how partisan the American process had become was revealed in July when the Koch-funded American Legislative Exchange Council, which represents nearly a quarter of mainly Republican state legislators, said “ No Thanks!” to federal support for states hard-hit by the pandemic.
At the same time that President Trump was assigning primary responsibility for meeting the emergency to the states, he was refusing the Democrats’ proposal to help state and local governments pay for the pandemic policies they implemented.
It probably was inevitable that face masks would become entangled in the presidential contest. In mid-August, Democratic candidate Joe Biden and his newly-selected running mate, Kamala Harris, kicked off their campaign by calling for a three-month face mask mandate.
In the midst of all this, most Americans, despite their widespread distrust of government and experts, rate information provided by the CDC more favorably than that provided by the Trump Administration. But still other Americans, some of them carrying highly-lethal weapons and waving confederate flags, have marched against governors, like Michigan’s Gretchen Whitmer, who had shut down their states’ economies to save lives.
Are the institutional weakness and policy confusion of the American response to the pandemic beyond repair?
Recent developments may offer some hope.
As often happens in times of emergency when central governments are paralyzed, groups of citizens have begun to stir. Sometimes, these groups are spurred by well-organized civil society groups, but often neighborhood groups, professional organizations, and ordinary citizens band together to fill the gap that governments leave open. (The “mad cow” episode in the UK was a good example. When the British government failed to respond to the threatened epidemic with effective measures or even clear information, civil society groups filled the gap.)
Early in August, 350 progressive public health groups signed a petition to end political interference in the CDC. Nurses and other first providers have expanded their protests against the inadequacy of the government’s response to support for people of color who have suffered most from the pandemic. As the school year began and cases of children testing positive began to mount, Florida’s teachers’ union began to mobilize against the opening of public schools with insufficient preparation. And in response to the Trump administration’s attempts to throttle the post offices just as early voting is set to begin, at least 12 professional sports teams from the worlds of baseball, basketball, football and hockey are offering their stadiums as places that can provide rapid, safe and socially distanced voting.
When the government fails to act, ordinary citizens begin to move. In this moment of general mobilization over the police murder of George Floyd, with a critical national election impending, and a quasi-paralysis of the federal government, more mobilization from below may be a last resort. But it’s also our best hope.
Isabel Perera is Assistant Professor of Government at Cornell University and author of articles that have appeared in both health and social science journals, including The Lancet Psychiatry, the American Journal of Public Health, and Politics & Society.
Sidney Tarrow is Emeritus Professor of Government at Cornell University and co-editor (with David S. Meyer) of The Resistance: The Dawn of the Anti-Trump Opposition Movement.