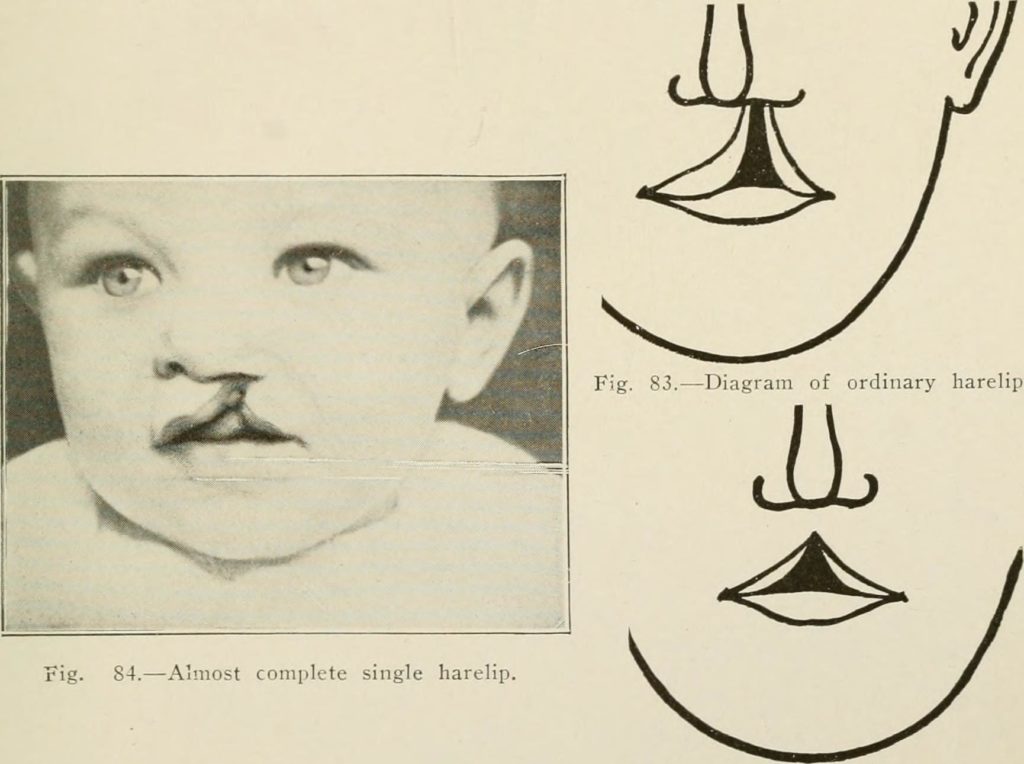
Photo Credit: Wikimedia Commons
When my mother was pregnant with my youngest sister, she went to consult a cleft jaw and lip expert in London. She lay down on the examining table, lifted her legs up and peered at the doctor as he glared at the black and white image. She had done these checkups before since I was also born with cleft.
The expert muttered to himself, shook his head and asked: “What have you done?” He scoffed. “I mean, what possible drugs could you have taken?” A second assumption hung in the air: the cleft would have to be corrected.
It was not uncommon, then or now, to blame mothers for fetal development that departs from what is considered “normal,” but it is worth noting at the outset that this one has numerous causes. Cleft lip and palate are a result of undeveloped facial tissues. Around day 23 of the fetus’s life, five (soon to become) “bones” fuse to create the structure of the face. One bone stretches down from the “forehead.” Two jaw bones, left and right, grow down to meet the two jaw bones that grow upwards.
Push your tongue against your palate and you will feel a ridge: that is the scar of the merging. When a child is born with cleft lip, jaw or palate, however, the fusion was incomplete. It can leave infants with a gaping hole that stretches from lip to nose. Cleft palate is the most severe of these conditions: it impacts the ability to eat, breath and speak. Lip and jaw cleft, however, which my sister and I were born with, lead to an aesthetic disfigurement, and sometimes a nasal tone of voice.
There are various causes for cleft. It can be one of a number of outcomes from drug abuse during pregnancy. It is thought to be mostly genetic, but appears unpredictably: parents with symmetric faces can have children with cleft, while asymmetric parents can produce children without it. My aunt, an orthodontist with an expertise in cleft, tells me that parents with no discernable risk factors, and no family history, can also produce children with cleft.
I can only presume that the doctor who accused my mother of harming her own child in utero was aware that cleft appears arbitrarily, but he nevertheless implied that my mother should be ashamed, for herself and for her unborn daughter. To save my mother, and anyone else, from having to see a child with a facial malformation, he recommended corrective surgery immediately after delivery, instead of waiting for three months, the therapeutic standard. Now, some surgeons even perform cleft lip and palate surgeries inside the womb, making the repair potentially invisible and preventing the parents from seeing their child as a disabled person.
This emphasis on parental blame and parental comfort provokes the question: Who are the surgeries of cleft palate for? What is it with the open face that disturbs culture? What are, as Sarah Ahmed would ask, the politics of happiness? And whose suffering is alleviated through these surgeries?
In The Cultural Politics of Emotion (2014) Sarah Ahmed argues that emotions are not psychological states without context, but cultural artefacts created in relations of value. The global North and its political economy are, Ahmed explains, driven by “a politics of happiness” that fend off disgust, discomfort and – most importantly –shame.
What were the possibilities for shame in my mother’s interaction with her physician? The doctor may have been disgusted by the sight of the ultra sound, and in turn, shamed my mother for making him feel it. But that shame extended to his presumption that she would be shamed by such a child, and that my sister, the cleft child, would herself grow up to feel ashamed of her appearance.
The inevitability of being shamed, or feeling ashamed, because of the responses of other people leads to the question: are corrective surgeries for the cleft child or for those who might observe them. When my 20-year-old sister, who knows I am writing about this, went for a consultation on her wonky nose – a residue of the cleft surgery, she explained to me how cleft children hid under their hoodies in the waiting-room. They were hiding and ashamed of themselves, she said. The subtext was clear: Are you saying that they shouldn’t have this surgery?
Similarly, my cousin, who did the same nose-surgery, explained that when she sees another person with cleft, she doesn’t want to affiliate herself with them. Shame is an affective response inflicted upon the subject, but it also encompasses preemptive responses to what others might think. Hide, hide, hide. You might be revealed as a freak.
But what about disgust, something that is rarely felt internally, and usually projected on an external object or person? Psychologists Paul Rozin and April Fallon argue that disgust is a form of “revulsion,” triggered by the potential ingestion, and vomiting up, of offensive objects, a confusion of exterior and interior that is a timeless and universal emotion. Following this argument, the need to conceal cleft lip is because the open lip reveals an interior, a disfigurement that would create an instinctive reaction of disgust from any observer.
Others understand disgust as an assumption, not a reality. Sarah Ahmed, for example, understands disgust as a cultural artefact that inhabits the boundaries of inside and outside. But she argues that this line between is negotiable, one that needs to be collectively agreed upon. Borders fluctuate. They move and are unruly, yet we try to control them – we might even be imposing disgust on them – in an attempt to know what belongs and what doesn’t. In this reading, a face shaped by cleft becomes a border object, instinctively human yet different.
From this perspective, the open, cleft mouth is not a disgusting object. It’s a line that confronts the viewer and asks: What are the possibilities for life?
Days after leaving the hospital with my newborn and “unrepaired” sister, my mother visited my primary-school. Passersby and teachers pulled towards the trolley and then back at the site of the baby. Some teachers expressed concern for their students. Would seeing this “unrepaired” human frighten them?
My mother doubted her decision to bring my sister into the public, disrupting the cohesion of normal faces. She entered the classroom. Seven-year-olds peered at the newborn, asked questions and held her fingers.
When I explain to adults that I was born with cleft lip, they often state that they had no idea, or that they don’t notice it. But, when I encounter a child, I’m struck by my own appearance: Why do you have a scar, or What happened on your lip? They immediately ask. Children are curious and seemingly more accepting to difference. They see the scar as a symbol of an event that demands causality, but they are not afraid.
Children don’t understand borders yet. As Ahmed notes, there is potential at the moments when the border between the inside and outside is negotiated, or when love emerges out of discomfort. My mother, by bringing my unrepaired sister to my school, was creating that possibility, and I want to believe it was a performative act that declared: With all your faces, you are loved.
Aside from potential difficulty breathing or eating, the reason for surgery is the assumption that uncorrected cleft children will be rejected by society. These surgeries can be traced back to 350BC in China, and the bones of discarded children with cleft lips can be found in most regions. Yet, in other societies, clefts are seen as blessings. Among indigenous communities in Central South America, the open mouth is viewed as a spiritual bridge to the animal kingdom, the Gods, and supernatural powers. Being born with a cleft lip in these regions is not just normalized or accepted but considered an opening into a world beyond.
But this view is challenged by global medical NGOs such as Operation Smile that have woven axiomatic corrections of so-called birth “defects” into a language of care. Operation Smile’s first trip was in 1982: today the organization has teams in 25 countries and has performed over 100,000 surgeries that it argues are urgent. “The majority of these children are unable to receive the medical care they need because it is too costly, far away, or specialized,” the website notes. “Because of this, being born with a cleft condition can be fatal. If a child survives, they may face bullying and social isolation.” Operation Smile Sweden explains the need for these surgeries in terms of a child’s happiness. “We could have been called Operation Survival, Safety, Confidence, Friends, School, Love, Hope and Future,” they write, “but that would be a bit long. So, we are called Operation Smile. And that’s what our work results into, more smiles.”
Accounts by plastic surgeons and other medical personnel speak to a missionary and almost spiritual experience working with the NGO. For example, the British nurse Jackie writes about a mother who was abandoned by her husband because of her son’s deformity. “He touched our hearts as all the children do,” Jackie wrote of the child in 2014. “As a mum and a nurse, I feel privileged to be part of Joshua’s journey and all the beautiful children Operation Smile helps around the world.”
The mission of NGOs like Operation Smile is to literally make children with cleft lip and palate smile. Technically though, this is not a medical achievement. Despite having a hole stretching from the lip to the nostril, children with cleft palate can smile and therefore succeed in fulfilling one of the most important functions of a face: to communicate emotions and establish relationships. Harriet Oster, who studied observers’ abilities to interpret the emotions of infants with facial anomalies, including uncorrected cleft lips, concluded in 2003 that the observers’ ratings were “highly accurate.”
How then, do we understand these surgeries as inherently urgent and necessary? Operation Smile’s agenda can perhaps be better understood as what anthropologist Miriam Ticktin has called a “politics of care” that helps to organize a structurally unjust postcolonial world. She connects this to the wave of new humanitarianism that the NGO Médecins Sans Frontières (Doctors without Borders) initiated in 1971. As Ticktin writes: “Rather than change the conditions in which people live and thereby improve human life on a broader scale, the focus is on alleviating pain in the present moment.”
Consequentially, since the politics of care focuses on alleviating immediate pain, rather than the conditions that are causing pain, recognizing and curing suffering becomes a paramount concern. For its donors and volunteers, the work of Operation Smile replaces disgust with positive feelings, without questioning why cleft needs to be corrected in the first place – anywhere in the world.
This is a question that troubles many assumptions – about faces, about feelings, and about how people live their lives with disabilities – and it would be naïve of me to not recognize that. I, for example, wouldn’t be able to access the spaces that encouraged me to write these words without a corrected face; and even I can be surprised by images of uncorrected clefts. I am startled by seeing myself. And the parents who bring their children to the NGOs want their child to be able to live on the side of the border I am now on.
Yet, erasing and assimilating difference also enforces ideals of normalcy and happiness that create borders in the first place. It marginalizes those who live in the borderland between inside and outside, people who will continue to exist. Because, despite all the technologies of repair that are produced to control us, we who are abnormal slip through. We leave traces in the form of scars and uncanny reactions. We remind the culture of its fragility.
Instead of assuming that correcting cleft is axiomatic, saves lives, prevents bullying, and creates happiness, what would happen if we said “no” – or even “maybe” – to a surgery that has become common-sense? Could we move towards a political order where to be “human” is to be on a broad and unruly spectrum? Where difference is valued instead of shamed?
Asking these questions could take us to a place where uncorrected children are honored, instead of hidden, and where our primary concern behind corrections is not how well can we hide a cleft, but what is lost if we do.
Ella Hillström graduated with an MA in Anthropology from the New School for Social Research.